
Explore the RHS Facebook Archives, a rich repository of local history written by Carol Flynn. For two decades, Carol brought a deeply dedicated voice to public education at RHS. Her role as Facebook administrator through mid-2025 naturally extended her prolific research into meticulously detailed articles, most notably her multi-part historical series posts. Today, Carol continues her local history writing for The Beverly Review and other outlets.
Spanish Flu Pandemic
Chicago – indeed, the entire world – has been here before.
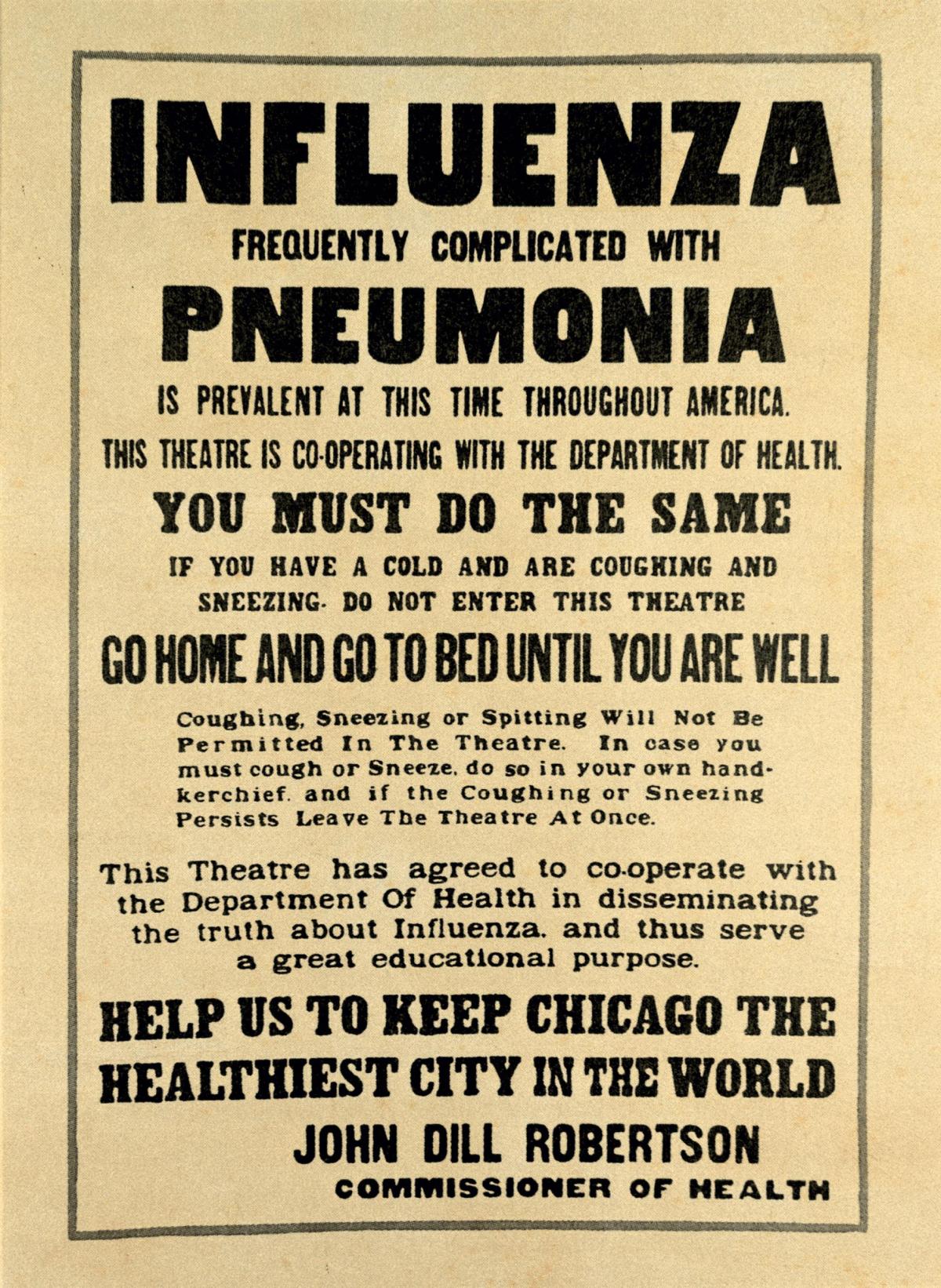
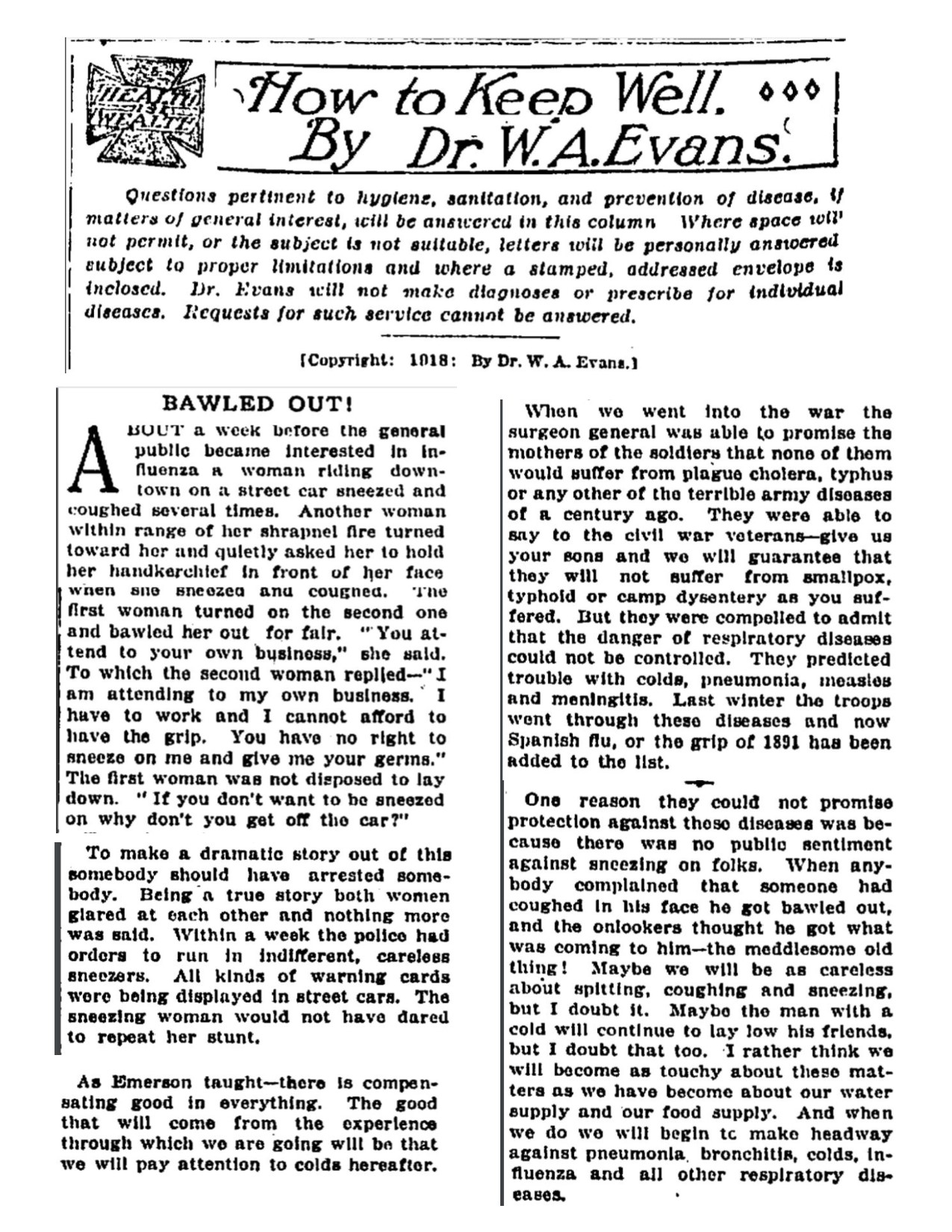
From Dr. W. A. Evans of the Chicago Daily Tribune: “Persons should avoid crowded assemblages, street cars and the like. Promiscuous coughing and spitting must not be tolerated. When a person comes down with the disease he should be cared for in well-ventilated, warm rooms as far as possible from other family members. The [disease] is spread by the nose and mouth secretions. These secretions are spread by coughing, spitting, sneezing, by the use of soiled handkerchiefs, towels, cups, spoons, and so forth. The folly of disregarding warnings [will be paid for].”
Sound familiar? Evans wrote these words about the Influenza pandemic in his Tribune column called “How to Keep Well” in the Fall of 1918.
The influenza outbreak that would eventually result in millions of deaths worldwide started in the military population of World War I and quickly spread to the civilian population. It was called the “Spanish Flu” but in fact, to this day, experts do not really know where this strain originated – some theorize it could even have started in the U.S. They also cannot agree on the total number of victims with estimates ranging from 17 million to 100 million. The world population at the time was about 1.9 billion. In the U.S., about 28% of the population of 105 million became infected, and 500,000 to 675,000 people died. These numbers are from the U.S. Department of Health & Human Services.
Increased travel for military personnel and civilians spread the disease. The disease was downplayed in the beginning to maintain the troops’ morale. It was first noted in Kansas in January 1918 when a Fort Riley cook reported sick, and within days, over 500 other men reported sick. The virus spread to New York City by March. Failure to take preventive measures then has been criticized.
By summer, the flu was in Chicago. Dr. Evans, among others, at first dismissed it as just routine annual “grippe,” the term they used then for influenza. Politicians and health authorities said it was all under control and would soon be over.
But it really started to explode in September and October. Strict quarantines were instituted at area military camps, including Great Lakes Naval and Fort Sheridan. Public funerals were stopped, in the belief people could become infected from the corpse; family members could only view the deceased though glass windows in the coffins.
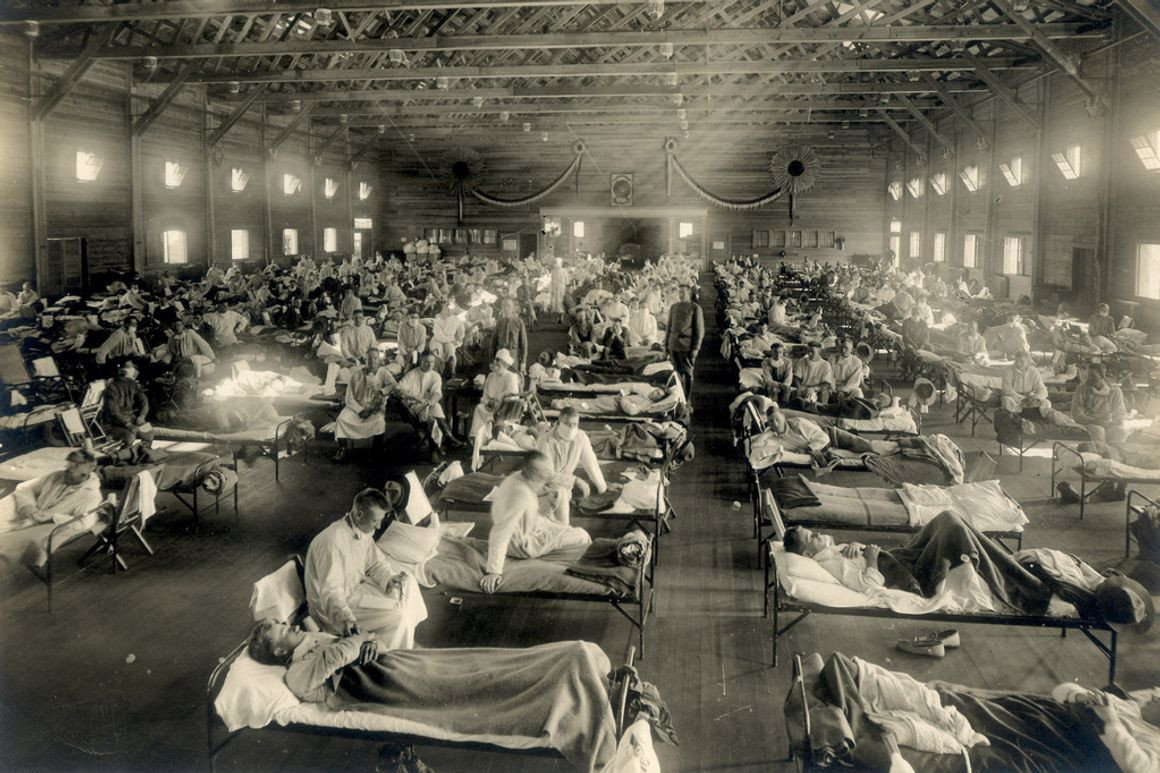
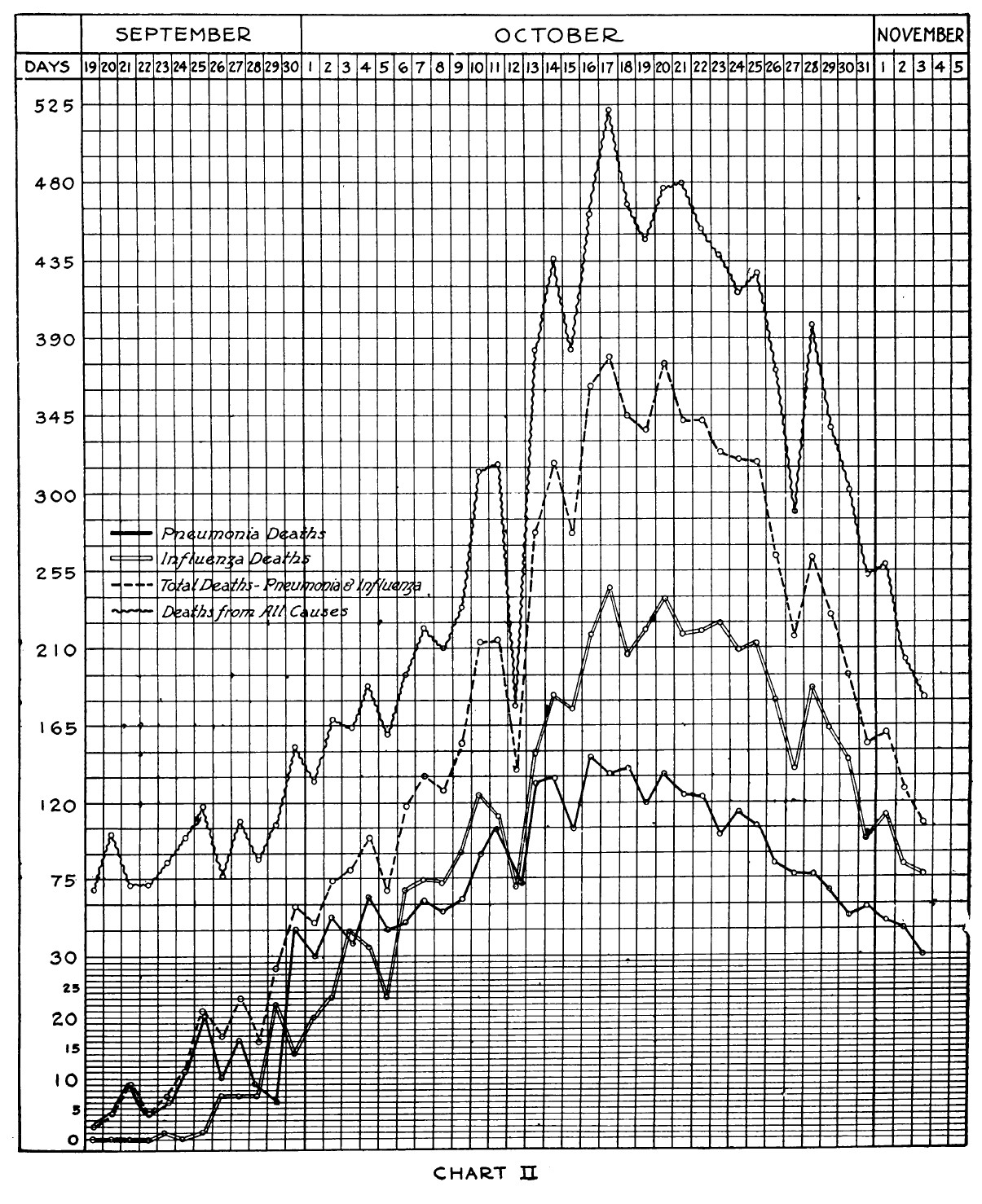
In Chicago, on October 3, 1918, there were 767 new cases of influenza and 355 cases of pneumonia reported, and a total of 119 deaths. The numbers were watched daily. On October 8, there were 1.342 new cases and 135 deaths. On October 15, there were 2,221 new cases and 317 deaths. There was a critical shortage of doctors, nurses and hospital beds.
A Catholic school was closed after a nun died of influenza. Chicago suspended public dancing in cabarets. The street cars were cleaned and smoking was forbidden. Conventions started cancelling.
A special “emergency commission” was put together to oversee Illinois efforts to combat the flu. On October 16, the commission announced that all theaters, lodges, night schools and skating rinks would temporarily close. The commission members could not reach agreement on churches, saloons, museums and other gathering places.
On October 17, the commission closed “nonessential-public gatherings” including athletic events, conventions, banquets and similar social affairs, parades, labor union meetings, political gatherings and cafes and cabarets.
Churches, saloons, pool halls and bowling alleys were exempt but were asked to exclude “sneezers, coughers and spitters” and avoid crowded situations. Some churches closed voluntarily. Later more activities and places were closed, including public playgrounds and swimming pools. Parents were instructed to keep their children home after school.
The Chief of Police ordered all violators of these rules be arrested. Arrests and busts were made, from smoking on street cars to “health raids” on overcrowded saloons.
Other suburbs took more drastic action. Oak Park closed schools and libraries. Evanston closed all churches.
Emergency kitchens were set up around the city to feed people affected by the pandemic.
Next installment: The flu continues ….
Part 2 – The influenza pandemic of 1918 continues in Chicago
In a Chicago Daily Tribune article on October 20, 1918, the business market was described as having “lapsed into a state of partial coma” due to the flu and news of the war.
Two treatments were being lauded for this influenza.
The first was a "preventive" vaccine developed by Dr. E. C. Rosenow of Mayo Clinic in Rochester, Minnesota. The initial group inoculated were doctors, nurses, police and other essential staff. Hundreds of thousands of Chicagoans were vaccinated, believing this would prevent them from getting the disease. In reality, this vaccine was useless against the viral influenza strain, which had not even been identified yet. There is some evidence this vaccine might have helped with secondary bacterial infections, such as pneumonia.
The second treatment, touted as a "cure," was a series of transfusions of blood from someone who had recovered from the influenza. Physicians bought blood to transfuse into their patients, believing in the immune properties of the anti-bodies built up by flu survivors. A modern review of this practice showed that it did seem to have some benefits in reducing mortality, but studies were not controlled by today’s standards for clinical trials. Blood transfusions are not considered practical in pandemics because of the number of infected people.
The city hired 100 women aged 50 to 60 to help with home nursing visits. It was believed that this population group was “an age practically immune to the disease.” People donated money to pay these women $15 per week.
Businesses and services suffered. Over 600 employees of the public transportation system were out sick and street cars and el trains went out of service with no repairs and maintenance, leading to even more crowding in the remaining cars. Businesses were not asked to close but to stagger their starting and ending times. Shopping was not curtailed.
The fiftieth annual (that’s right, FIFTY years) convention of the Illinois Equal Suffrage association went on as planned at the Congress Hotel. They followed the rules of the State Council of Defense and health authorities. They limited attendance to 100 delegates, the general public and the press were barred, and chairs were spaced four feet apart. The were criticized for not wearing masks.
As numbers of new cases and deaths decreased, restrictions were lifted. On November 10, the public health commissioner declared the epidemic in Chicago over, and lifted bans except for smoking on public transportation and refusing admittance of sneezers, coughers and spitters. Dr. Evans told the public in his column that they should expect several years of outbreaks as the flu is a “lingering disease.”
In early December, the commissioner reversed his course of action, claiming he never said the epidemic was over. New cases and deaths were once again on the rise. Restrictions were put back in place. He blamed the pharmacists for selling cough medicine with opiates that deadened the symptoms, and theaters for allowing in sneezers, coughers and spitters.
The American Public Health Association met in Chicago and formed committees to study and make recommendations for combating a recurrence of the flu. The three-day meeting ended without any consensus being formed and a group of five doctors including Dr. Evans were appointed to continue to work on the problem.
On December 15 it was recommended that people wash their hands frequently and stop shaking hands.
Christmas came and went quietly, overshadowed by the war and the flu pandemic.
Next installment: 1919 starts off with the flu

Part 3 – The influenza pandemic continued into 1919.
Restrictions from the influenza pandemic pretty much came to an end in Chicago by January 1919 except for the ban on smoking in public transportation cars. Night classes, plays, meetings, church activities, etc., all resumed. New influenza cases and deaths continued but not at the rate of the previous Fall.
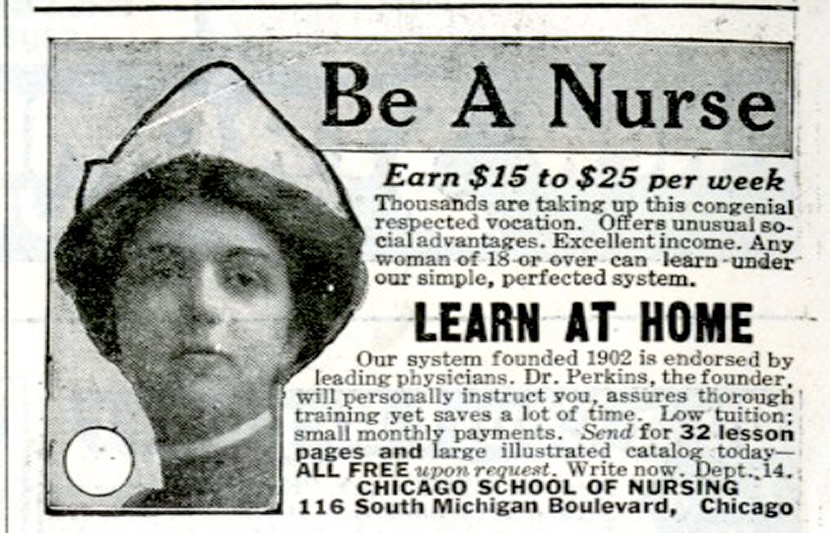
On January 12, the health commissioner, Dr. John Dill Robertson, authored an article in the Chicago Daily Tribune calling for an overhaul of the nursing profession. He stated that many of the influenza deaths could have been avoided with proper home nursing care, but there was a shortage of nurses. He maintained that the three years of training to become a Registered Nurse (R.N.) was too long, and that the $35 per week that R.N.s charged for home nursing care was more than could be afforded by middle class families.
Robertson wrote of nurses: “It has been well said that women are natural nurses. This is true. As a matter of fact, the principal business of a nurse is to follow the doctor’s instructions…. Of course she should have training; but it is difficult to see why a three year course of training is necessary before a nurse can be trusted in the sick room of the home…. In the final analysis nursing is nothing more or less than housekeeping for the sick.”
He called for establishing a two-tier nursing structure: R.N.s, and “practical” nurses, with less training, who could do home care at half the salary of R.N.s.
Physician and hospital groups immediately supported this new nursing plan.
Most R.N.s and their organizations were against this, fearing it would lessen the profession.
Wrote Edna L. Foley, the head of the Visiting Nurses Association: “…There are no over trained nurses, but there are too many poor training schools…. The education of a nurse has become more complex and involved because the advancement of medical and surgical science made better trained and more skilled nurses necessary…. Private duty nursing in the home is the hardest, least attractive type of nursing work…. The household nurse, the neighborhood nurse, the practical nurse, or the attendant, as she has been variously called, is a combination devoutly to be wished for, a kindly, capable, practical person, useful in the sick room, equally useful in a kitchenette or in the nursery: a woman able to be on duty from twelve to eighteen hours a day, and on call at night; a woman who is a good housekeeper as well as a sick room caretaker.”
For three months debates about this went on. The nurses came to support a one-year training program for practical nurses and a two-year program to become an entry-level R. N., with testing and licensure for both. It was recognized on all sides that a nurse specializing in certain areas, such as surgery or obstetrics, or acting in a supervisory role, needed advanced training. In April 1919, the Illinois legislature passed a bill establishing the two levels of nursing.
The health department discovered physicians had written over 100,000 prescriptions for narcotics to treat influenza in the month of October 1918. Pharmacists routinely carried and dispensed opium, morphine, codeine, heroin and cocaine. The danger was that the drugs suppressed the symptoms of the disease, especially coughing, and led to an increase in pneumonia, as well as dependency. Physicians were advised not to prescribe narcotics. The Chicago Retail Druggists’ Association was outraged and passed a resolution condemning what they considered to be an attack on retail pharmacy.
People were warned not to kiss babies to avoid giving them germs, and public school students were advised to avoid soda fountains unlss they used paper cups.
In his February 23 Tribune article, Dr. Evans wrote of the influenza pandemic: “Efforts made by health departments to control the disease have not been satisfying to them nor the public. The efforts of the research men to find the bacterial cause of the disease and the method by which it is spread likewise have proven disappointing. These failures and disappointments in the control of so severe an epidemic have caused much speculation.”
The insurance companies reported they paid out over $2.5 million in the U.S. due to the pandemic, which led to an increase in premiums.
Next installment: Summer finally arrives in Chicago.
Part 4 – The summer of 1919 finally arrived, bringing a respite to the influenza epidemic in Chicago.
On June 24 the city council lifted the ban on smoking on the el and street cars.
Dr. Evans, the columnist in the Chicago Tribune, was against this – he wrote that the epidemic was not over, no epidemic had lasted less than two years.
Evans wrote that the bacteria, which they thought the flu was, would remain virulent for 5 to 10 years. He commented that safety had been in the precautions that were taken and to let down the guard now could still result in trouble. He mentioned that smallpox was still an issue after many years.
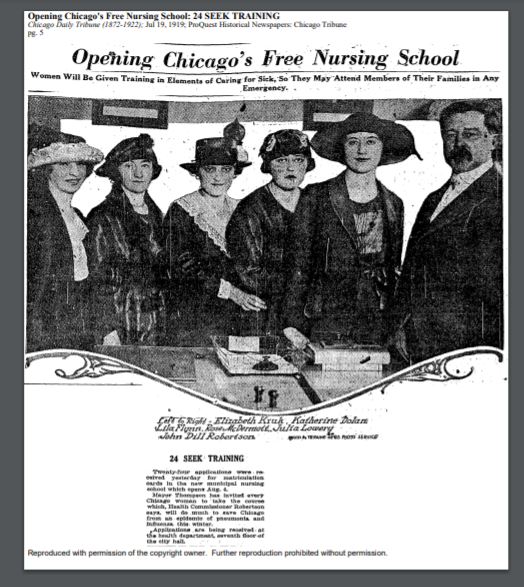
On August 4, 800 women started training as nurses in a new school set up by Dr. Robertson, the public health commissioner. This was an eight-week program to train home and public health nurses. They graduated on September 30th and another class began immediately. A register of the graduates was kept at the health department.
In late August/early September, deaths from influenza began to rise again. People were reminded of flu precautions.
Dr. Evans recommended that people be vaccinated, but he did state that it was now believed influenza was caused by a virus, not by bacteria, and that the vaccine could help reduce the risk of getting pneumonia.
Pollution was becoming a big issue, and it was recognized that smoke pouring into the air was exacerbating lung illnesses such as pneumonia. Armour & Co., the meat packer, was ordered to shut down furnaces that were causing pollution in the city. Over 111 violations had been reported against Armour since 1917, and fifty suits filed against the company.
But 1919 was a much milder year for the flu. In November, there were 178 new cases and 26 deaths compared to 4,177 cases and 1,155 deaths in 1918. For pneumonia, there were 610 new cases and 192 deaths compared to 2,490 cases and 639 deaths in 1918. Bigger concerns in 1919 were measles, chicken pox, mumps, whooping cough, scarlet fever and diphtheria.
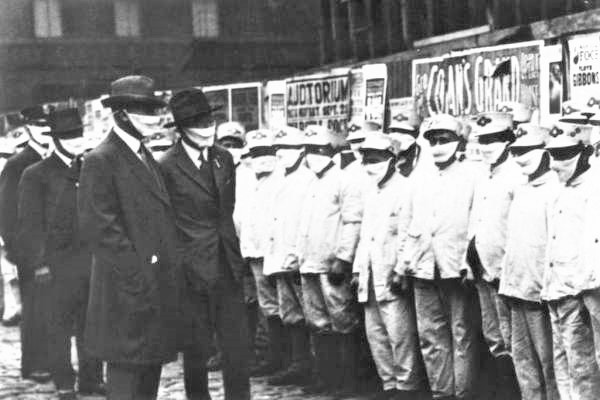
Chicago didn’t do as badly with the influenza pandemic as some other cities did. Credit for this was given to the preventive measures and restrictions put in place.
In 1917, the overall mortality rate for the U.S. was 14.2 per 1000 people; this rose to 19.6 in 1918 due to the influenza outbreak. In Chicago, with a population of about 2.5 million people, the 1917 mortality rate of 14.9 per 1000 rose to 17.1 in 1918. Other cities had much higher rates – Baltimore rose to 26.8 and Nashville to 26.4, the highest increases.
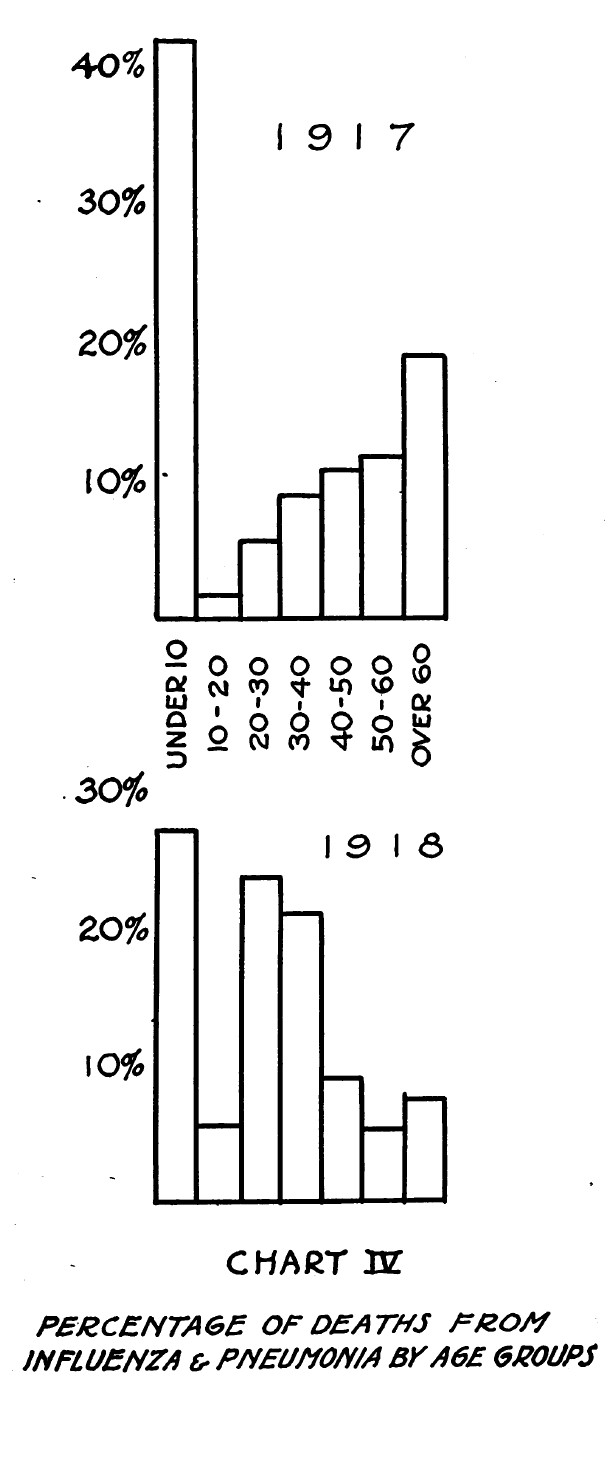
The hardest hit population group was adults aged 20 to 49. One thing noted about the flu was that survivors reported complete recovery with very few after effects.
Note that scientists now classify the 1918 influenza, aka the Spanish Flu, as a strain of Influenza A virus subtype H1N1 (A/H1N1). This was an unusually severe and deadly strain of avian influenza, a viral infectious disease. Another H1N1 strain caused the 2009 pandemic. The annual flu vaccine typically gives coverage against several strains of H1N1.
Viruses are the most prevalent biological entity on earth, found in almost all ecosystems. Of the millions of viruses out there, about 5,000 have been described, and of these, at least 220 can infect humans.
Last installment: Some flu-related “good news” stories.
We’ll call this installment Part 4B because this research document is just too good to pass up.
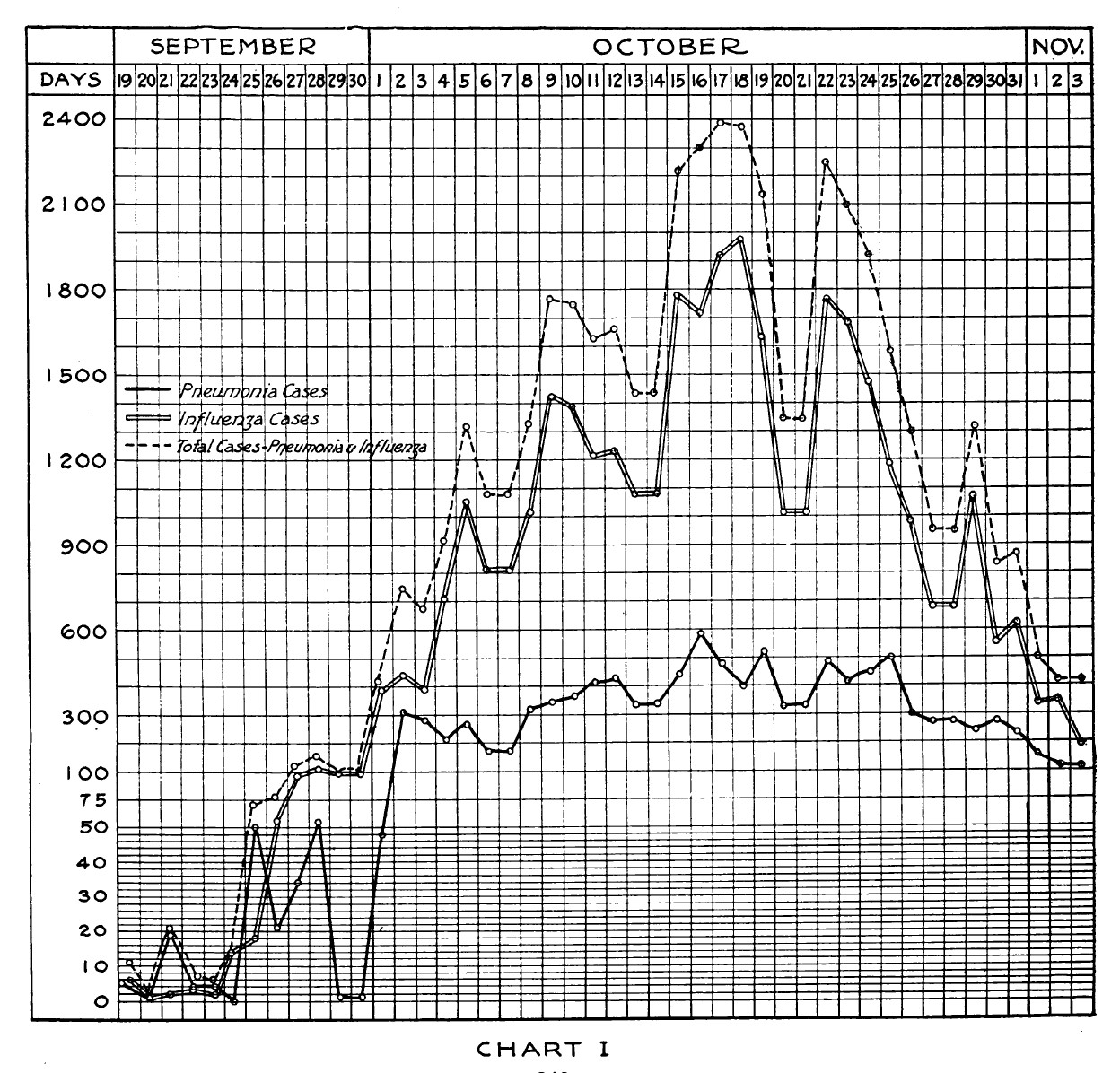
In November 1918, Dr. John Dill Robertson, the Health Commissioner for Chicago, published a “Preliminary Report on the Influenza Epidemic in Chicago” in the American Journal of Public Health.
In this article, he gave statistics about the disease in graphical form for the month before, October 1918, which would prove to be the worse month for the outbreak. Three of those graphs are posted here.
He also gave a chronology of the measures employed to control the epidemic. Some highlights were:
September 17 – Proclaimed influenza a reportable disease [first cases reported in the city]
September 21 – Issued warning to the public about the symptoms and self-quarantine at home
September 26 – Started inspection of schools and students
September 30 – Started daily disinfecting of public transportation cars
October 1 – Started quarantine of influenza patients in hospitals and homes
October 4 – Procured home nurses from Visiting Nurses Association
October 5 – Started warnings about public gatherings (churches, etc.)
October 11 – Procured more home nurses from other organizations
October 12 – Closed public dance halls; prohibited public funerals; added 150 full-time “health officers” to the city payroll; met with leaders of 40 civic organizations to assure cooperation
October 13 – Banned smoking on public transportation cars
October 15 – Closed theaters, skating rinks, night schools and lodge halls
October 17 – Ordered businesses to stagger starting and ending times; announce vaccination program
October 18 – Stopped all non-essential public gatherings
October 19-20 – Reviewed hospitals for available space; stopped all elective surgeries
October 21 – Recruited additional home nurses
October 22 – Received vaccinations and started program
October 23 – Met with laboratories to produce immune human serum
October 29-30 – Began lifting ban on public gatherings
November 4 – Lifted remaining bans on public gatherings
Part 5 – Every cloud has a silver lining
Part 5a – Every cloud has a silver lining
Our final installments about the 1918 influenza pandemic in Chicago is a story about how the lives of real people were affected.
It was October 16, 1918. Mrs. Alice Proctor, 34, was a patient at Mercy Hospital, suffering from influenza. She had moved to the United States from England two years before with her husband and son. Her husband had died, leaving her alone with her son Sanford, now 6. The week before, Alice had been hired as a maid by the George A. Rees family in Hyde Park. The second day on the job, both she and Sanford were put to bed sick at the employer’s house. Alice’s symptoms worsened and she was hospitalized.
Sanford, still at the Rees home, was being treated for double pneumonia following influenza. He had previously suffered from “infantile paralysis,” the term for polio, which had left one leg crippled. He was described as “the most patient and pleasant little fellow in the world.”
Alice knew she was dying. She had no family, and she was worried about what would happen to her little boy. She asked the hospital staff to help her contact the Chicago Daily Tribune. She then asked the newspaper if they could help her find a home for her little boy.
A reporter, never named in the newspaper, consulted a lawyer acquaintance, Charles L. Phillips, who agreed to help. They visited Alice at the hospital and worked out the details whereby she would leave her child and her precious few personal belongings to the family who would adopt Sanford.
“I am glad,” she whispered faintly, “and I can die happy.”
In the next few days, Alice rallied. and it was thought she might survive. But she died on October 19th.
In the meantime, Sanford had been admitted to St. Luke’s Hospital. He asked for his mother. He didn’t understand where she was and why she was not coming to see him. The hospital staff did not tell him she would never return.
The Tribune put out a call for families who might adopt Sanford Proctor. Perhaps a family who had lost a son in the war, suggested the paper, or a couple who had not been blessed with children of their own.
Alice’s employers, Mr. and Mrs. Rees, were fond of Sanford, but they already had three children of their own. They did want the child to convalesce at their home and were concerned that a good family be found for him.
Sanford brightened the ward at St. Luke’s, but he wanted his mother.
“I hope my mamma gets well soon and comes to see me,” Sanford told the reporter. “I like the nurses but I like my mamma better. Will you tell her I am getting well quick so I can see her?’
Offers to adopt the boy poured into the Tribune. People were instructed to put in writing their ability to care for the child.
Responses came from the wealthy who promised very fine homes and from poorer families who promised love. Country folk and city folk and suburban folk responded. Attorneys and farmers responded. The mayor of a city in Michigan responded. People who had lost children and people who had children for Sanford to be a brother to responded. Special pleas came from childless couples and from Gold Star mothers who lost sons in the war. People promised Sanford would receive everything from fresh air, sunshine and fun to church attendance to medical care to a good education.
The Tribune narrowed the possibilities to twenty-four potential families that were being investigated. Sanford improved and was expected to be released from the hospital to the care of the Rees family, where he would meet with prospective new parents.
On November 5th, the reporter wrote that Sanford would be released from the hospital within days, and that he would soon learn that his “mommers,” for whom he asked constantly, was dead and he was an orphan. The choice of new parents had been narrowed down to a select few. And Sanford would receive a bill for $100 for his mother’s funeral and burial.
Next installment: Little Sanford Proctor gets a new home.

REVISED, and then REVISED again
Part 5b. Little Sanford Proctor finds a new home.
Sanford Proctor was a six-year old boy whose mother died of influenza during the 1918 pandemic. Having already lost his father, Sanford was now an orphan. On her deathbed, his mother had contacted the Chicago Daily Tribune to ask for help in finding a home for her son. Scores of people contacted the Tribune with offers to adopt the boy.
On November 16, 1918, the Tribune announced that Sanford had a new home. The doctor who had been treating Sanford at St. Luke’s Hospital had obtained custody of the little boy.
This doctor, whose name was not revealed in the article, had cared for the boy daily, often neglecting his outside practice to do so. Not only was Sanford’s pneumonia on the mend, the doctor also believed that expert care would help his crippled leg.
The doctor and his little patient had become great friends. When the time came for Sanford to be discharged from the hospital, the doctor realized he could not watch Sanford go.
“I can’t think of letting my little companion go into another’s home,” said the doctor. “I have grown attached to him. I can cure his shriveled leg and make a fine young man out of him.”
The article reported that Sanford would be going to a fine city residence and a spacious country home where he could romp and play. The doctor and his wife intended to adopt the boy and give him their family name.
Who was this kind-hearted physician? The story wouldn’t be complete without further research. This happened in 1918, so the assumption was made that Sanford should be in the 1920 U. S. Census under his new name. A search through the census records on Ancestry.com for Sanfords in Chicago in 1920 found him – he was now Sanford Watkins, living at 4943 S. Blackstone Ave., one of the finest addresses in the entire city.
Sanford was adopted by Dr. Thomas James Watkins and his wife Catherine. Dr. Watkins was head of the gynecology department and a professor of medicine at Northwestern University. He was also one of the heads of St. Luke’s Hospital and affiliated with Mercy Hospital. He was a past president of the American Gynecological Society and a presenter and author of renown.
Research also found that Thomas and Catherine Watkins had lost their only child, a seven-year old boy named Carman (Catherine’s maiden name) in 1901. The child was buried at Mt. Hope Cemetery on 115th Street here on the Ridge.
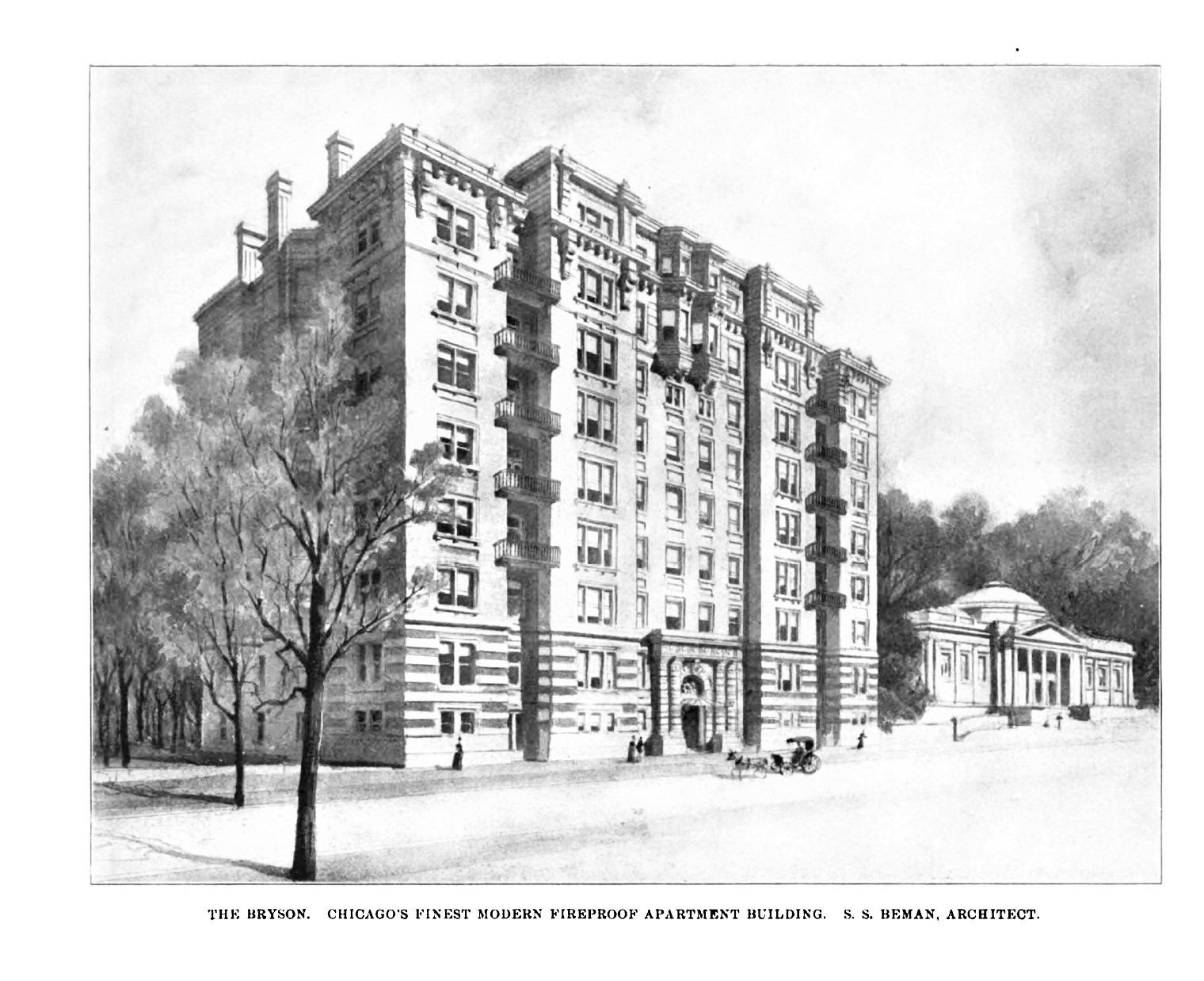
Dr. and Mrs. Watkins and Sanford lived at the Bryson Apartment Building, one of Chicago’s exclusive, grand buildings where the apartments had eleven huge rooms, soaring ceilings and marble entryways. The building, which no longer stands, was sold in 1923 to be turned into a hotel. The Watkins family moved to another fine new apartment building on Chicago’s Gold Coast at 219 East Lake Shore Drive, which today houses multi-million-dollar condos.
Dr. Watkins died of a heart attack at his office in 1925 at the age of 62. His remains were returned to New York where he was from originally. At the time of his adopted father’s death, Sanford, 12, was a student at St. John’s military academy in Wisconsin. Dr. Watkins left a trust fund of $50,000 for Sanford, which would equate to more than $700,000 in 2020.
We found further information on Sanford. In the early 1930s, he was a student at the University of Illinois – Urbana. For a while, he lived in rooms at the South Shore Country Club, where he was an avid golfer.
It appears he spent time in New York in the mid-1930s. He did travel from New York to England and Germany in the early 1930s.
The 1940 census found Sanford, 27, with his wife Barbara and son Thomas James, presumably named for Dr. Watkins, living in Beverly Hills, California. His occupation was listed variously as writer and stenographer.
Barbara was the daughter of Charles Helsell, an executive with the Illinois Central Railroad. The Helsells lived in Flossmoor.
On his 1940 draft registration card, Sanford listed his employer as John Truesdell. Truesdell was a young man in his late 20’s from Ohio who wrote a Hollywood gossip column that was carried by several Midwest newspapers. We’re assuming that Truesdell dictated his material to Sanford who transcribed it for publication.
Alas, though, we are sorry to report that Sanford died in December 1941 in California, at the age of 29, leaving a young widow and baby son. We are researching the death certificate to learn the cause of death.
We found that Barbara remarried in 1957 to John Whit Foster. Barbara died in 2003 in San Diego. Barbara’s and Sanford’s son Thomas James died in 1996. We do not know if he left descendants.
So many stories of individuals from the influenza pandemic of 1918-1919 had sad endings. It was nice to find this one “feel good” story from the 1918 Tribune about the orphan Sanford Proctor. And it looked like life was going well for Sanford for a time. In a twist of fate, just as Sanford never knew his father, his son never knew him.
We’ll do one more post to look at some miscellaneous stories and information about the 1918-1919 influenza pandemic in Chicago.
Part 6: What happened to the Spanish flu, and some things never change
The “Spanish Flu” infected the world’s population from 1917-1920. Then it pretty much just disappeared.
At the time, no one really knew what viruses were. They knew there was something smaller than bacteria that could not be seen even with microscopes. They knew these pathogens could infect, be transmitted between, and cause grave illnesses in humans. They knew viruses needed living cells as hosts unlike bacteria that could be cultured in a nutrient medium. Some illnesses they knew resulted from viruses included rabies, polio and influenza.
1931 saw big breakthroughs. The electron microscope was invented allowing ever smaller sub-microscopic matter to be viewed. Influenza and other viruses were grown in fertilized chicken eggs. This led to the “golden age of virus discovery” which has resulted in where we are now in identifying viruses and treating the illnesses they cause.
In the 1990s, the strain of influenza that caused the 1918 pandemic was extracted from old tissue samples. The virus, kept in secure laboratories with top level clearance for admittance, is used for research. One conjecture as to why the virus “disappeared” from humans is that the structure of the virus mutated, or changed, into a less lethal form.
There are many similarities between the 1918 influenza pandemic and the 2020 coronavirus pandemic. Certainly one example is the reaction of some people to taking precautions not to spread the contagion.
This Chicago Daily Tribune article from Dr. Evans is a timely reminder that some attitudes from then are still around today. Some things have not changed – but maybe they will this time.
Chicago Daily Tribune, October 22, 1918